
Hair transplant procedures have gone through a number of major evolution, beginning in the early 1900s in Japan and progressing to today, with research continuing. Hair restoration surgery by transplantation has evolved into a more and more cosmetically acceptable procedure, moving through the early punch grafts and mini and micrografts to the most current follicular unit extraction or FUE
Earlier Hair Transplant Methods
The first hair replacement method was based on the punch graft. This was originally attributed to the American Dr. Norman Orentriech, however it is now generally accepted that this technique was used earlier by Japanese dermatologists. Dr. Shoji Okuda first used the punch micrograft in 1939 on the scalp, mustache and eyebrows. In 1943, a paper by Dr. Hajime Tamura detailed the use of elliptical excision, akin to the modern strip excision procedure and foreshadowing the trend toward smaller and smaller grafts. In 1952, Dr. Orentreich popularized the punch graft using 4mm punch grafts. This was the standard until the mid ‘70s, but gave an unpleasant “doll’s head” appearance. When hair was lost around the graft “plugs” became visible. Unfortunately, for decades that followed, the general populace equated hair transplant results with the doll’s head look.
|
|


Dr. Orentreich also originated the theory of donor dominance, where hair taken from the back of the hair and transplanted to the front continued to grow, thus exhibiting the behavior of the donor hair. “Donor dominance” is a theory currently undergoing modification due to experiments in the field that show donor area might not be the sole determining factor. Dr. Umar believes that some characteristics such as graft survival is innate in the hair itself and that the place it is pulled from plays only a secondary role.
Los Angeles Hair Transplant Surgery Methods Today
Strip excision also known as follicular unit hair transplant – FUHT or follicular unit Strip Surgery – FUSS is the most commonly practiced method of hair transplantation today, with an elliptical strip donated from the back of the head and split into smaller grafts. The best donor area is right above the occipital bump or below an imaginary line that runs 1cm above the top of the ears. This invariably leaves a linear scar with a chance of stretching.



If the width of the incision is less than 1cm, it would reduce the chances of strip scar complications. Tricophytic closure is a recent innovation that gets hair to grow through the scar. In this procedure, a 1mm ledge of the outer layer of skin is cut off as well as an edge on the donor site before the wound is closed. This results in a smaller and less apparent
Hair Transplant Surgery in Los Angeles by Follicular Unit Extraction – FUE
Follicular Unit Extraction entails the extraction of individual follicular units one at a time directly from the back and sides of the head using 0.8 – 1.2mm punches. Unlike FUSS, there is no linear scars created in this technique, making it ideal for those who prefer to have short hairThis procedure does not leave any of the linear scarring associated with traditional strip graft surgery. Rather, the FUE method leaves very small wounds that heal with no significant scarring. There are two types of FUE hair transplant:
- Basic FUE which has some limitations
- Advanced FUE by UGraft which is engineered to overcome the challenges of basic FUE
Read more about FUE hair restoration in this article of which Dr U is a pioneer
This surgery gives an overview of some of the differences between Basic FUE and Advanced UGraft FUE:



Hair Transplant Surgery in Los Angeles: FUE VS FUSS
Here is a video illustrating the difference between follicular unit extraction – FUE vs FUSS also called follicular unit strip surgery:
Hair Transplant Surgery in Los Angeles : What Tomorrow Holds
Many automated hair transplantation machines are in the market today. Examples include the Neograft and the more robotic Artas. The Neograft incorporates a punch mounted on a rotary device as well as an optional suction device that removes the grafts as they are cut free from surrounding tissue. Concerns have been raised about the desiccating effect of the suction in Neograft which could result in graft damage. Artas as presented in the latest ISHRS meeting in the Bahamas, is a true robot that comes with computer enables sensors that enable the robotic arm to determine which grafts to dissect. The physician can participate in this process as well. However, the patient would have to keep still once positioned and has to be re-positioned every time the robot is done with a one given area. The physician would still need to remove the grafts manually after the robot has made the incisions which separate the hair follicle from it attachments. No suction is used. Read more about the Artas robot here
For physicians seriously considering adding FUE to their menu and services, even with the aid of the aforementioned machines, Dr Umar advises spending some time in training with Experienced FUE practitioners.
Hair Cloning and Hair Transplantation
One of the most exciting developments in the world of hair transplantation is the idea of cloning hair. The hope with hair cloning is to remove the limits placed by the donor area. A single biopsy punch could restore hair to the entire head, removing the fears of running out of donor hair.
Current Issues in Hair Restoration
A hair transplant procedure today is quite different from their invention in turn of the century Japan. Grafts are smaller, techniques are more precise and problems such as unnatural appearance have been resolved. New technologies present new issues, however, such as automation and genetic developments.
One of the most important details in a hair transplant surgery is the hair line. Others can often tell if a person has had some type of hair loss procedure based on just looking at the edge of the hair that borders the face. For more information on hair line transplant, click here to read more.
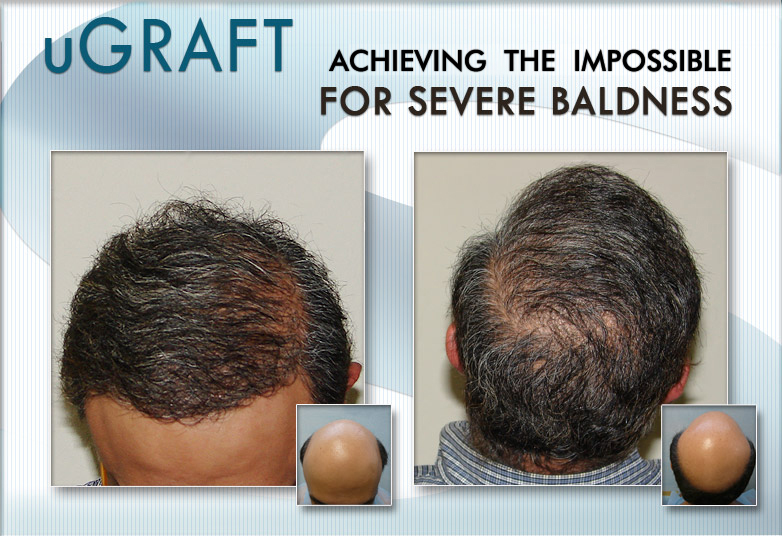
Hair Transplant Surgery in Los Angeles : Examples of Dr Umar’s Patients



If you are suffering from hair loss and wish to get a surgical hair restoration the first time around, feel free to consult Dr Umar using this free online consultation form
Related material
When would I see results of my hair restoration surgery
video explaining the FUE hair restoration process
What is the reason for poor growth after surgical hair restoration